 7430923244
7430923244



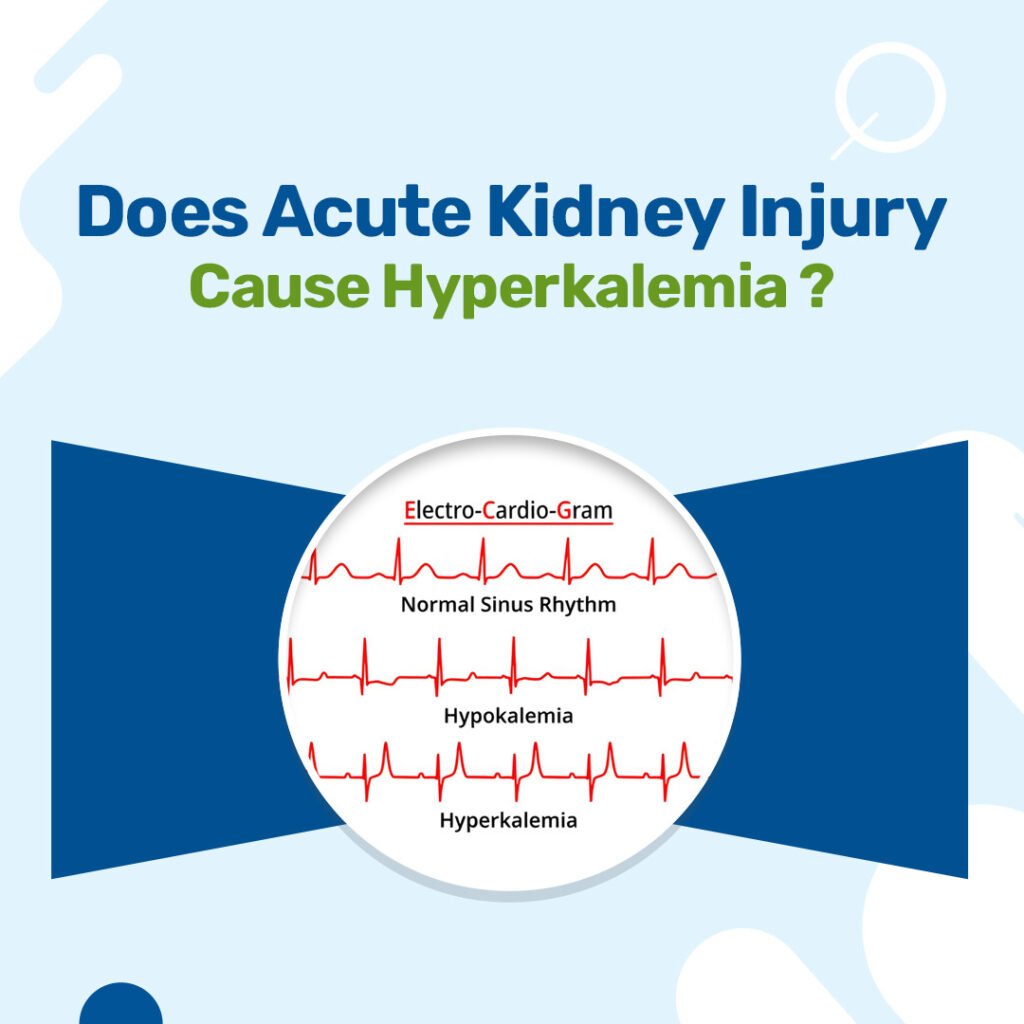
Yes, acute kidney injury commonly causes hyperkalemia and is considered one of the most serious electrolyte complications of AKI. Hyperkalemia occurs in AKI because the damaged kidneys lose their ability to adequately excrete potassium, leading to dangerous accumulation in the blood. According to medical literature, hyperkalemia is one of the major electrolyte disturbances in patients with acute kidney injury and severe hyperkalemia (serum K+ of at least 6.5 mmol/L) is particularly dangerous.
What Is the Most Common Electrolyte Imbalance in Acute Kidney Injury?
Hyperkalemia is the most common and dangerous electrolyte imbalance in acute kidney injury. In all cases of AKI, the most serious electrolyte disorders are hyperkalemia and fluid overload, which can potentially cause pulmonary edema. According to research, hyperkalemia is the most common electrolyte disturbance observed in patients with kidney disease, particularly in those with diabetes and heart failure or those on treatment with renin-angiotensin-aldosterone system inhibitors.
Other common electrolyte abnormalities in AKI include metabolic acidosis, hypocalcemia, and hyperphosphatemia. The most common complications related to electrolyte disturbances are hyperkalemia, hypernatremia, hypermagnesemia, and hypocalcemia. However, hyperkalemia remains the most clinically significant due to its potential for life-threatening cardiac arrhythmias.
Which Kidney Disease Causes Hyperkalemia?
Both acute kidney injury and chronic kidney disease can cause hyperkalemia, but the mechanisms and prevalence differ. Hyperkalemia is a frequent metabolic alteration in CKD patients that increases in the presence of drugs with beneficial cardio-renal properties. In chronic kidney disease, hyperkalemia prevalence increases with declining kidney function, affecting up to 50% of patients with advanced CKD.
| Kidney Disease Type | Hyperkalemia Prevalence | Risk Factors |
| Acute Kidney Injury | Very common in severe cases | Reduced GFR, decreased urine output |
| Chronic Kidney Disease | 15-50% depending on stage | RAAS inhibitors, diabetes, heart failure |
| End-Stage Renal Disease | Up to 80% | Dialysis timing, dietary factors |
Does AKI Cause Hypercalcemia?
AKI typically causes hypocalcemia initially, not hypercalcemia. According to medical literature, hypocalcemia occurs in AKI because the impaired kidney no longer produces calcitriol (reducing calcium absorption from the gastrointestinal tract) and because hyperphosphatemia causes calcium phosphate precipitation in tissues. However, during the recovery phase of AKI, hypercalcemia can occur due to mobilization of calcium phosphate deposits, affecting up to one-third of patients.
The relationship between calcium and AKI is complex: both very high and very low serum ionized calcium levels are associated with increased risk of developing AKI in hospitalized patients, showing a U-shaped curve relationship. Severe hypercalcemia can actually cause AKI through mechanisms such as volume depletion from polyuria and direct alterations of renal vascular tone.
Why Do Some AKI Patients Develop Hyperkalemia While Others Don’t?
The development of hyperkalemia in AKI patients depends on several factors including the severity of kidney dysfunction, underlying causes, and individual patient characteristics. Hyperkalemia occurs when renal potassium excretion is limited by reductions in glomerular filtration rate, tubular flow, and distal sodium delivery. The normal physiological response to volume depletion drives upregulation of aldosterone synthesis, so reductions in these parameters are normally offset by increases in aldosterone activity.
Hyperkalemia ensues when this compensatory response is prevented, for example by renin-angiotensin system inhibitors or mineralocorticoid receptor blockers. Additional factors influencing hyperkalemia development include:
- Severity of AKI: More severe kidney injury with greater GFR reduction leads to higher hyperkalemia risk
- Underlying cause: Rhabdomyolysis and tumor lysis syndrome cause massive potassium release from cells
- Medications: ACE inhibitors, ARBs, and potassium-sparing diuretics increase risk
- Comorbidities: Diabetes, heart failure, and acidosis predispose to hyperkalemia
- Patient factors: Age, baseline kidney function, and body weight affect susceptibility
What Is the Most Common Cause of Acute Kidney Injury?
Prerenal causes are the most common etiology of acute kidney injury, accounting for approximately 60-70% of cases. Prerenal AKI results from functional adaptation to hypoperfusion of functionally normal kidneys. The most common prerenal causes include hypovolemia secondary to excess fluid losses, diuretic use, or hemorrhage, impaired cardiac function leading to decreased effective circulating volume, and systemic vasodilation from sepsis, anaphylaxis, or anesthesia administration.
According to medical literature, prolonged renal ischemia, sepsis, and nephrotoxins are the most common overall causes of AKI. In hospitalized patients, the predominant etiologies include sepsis (22.4%), trauma due to road traffic accidents (21.18%), acute abdomen conditions (18.64%), and cardiac diseases (10.59%). Intrinsic causes, particularly acute tubular necrosis, represent the second most common category, while postrenal causes from obstruction are least common.
How Can You Treat Hyperkalemia from AKI in Siliguri?
In Siliguri, comprehensive hyperkalemia treatment from AKI is available at several specialized nephrology centers.
Treatment approaches for hyperkalemia in AKI include immediate cardiac stabilization with calcium therapy, shifting potassium into cells using insulin-glucose or sodium bicarbonate, and removing potassium from the body through dialysis or potassium-binding resins.

Dr. Vishal Golay runs a comprehensive nephrology practice at Remedy Clinics and Balaji Healthcare in Siliguri. The practice specializes in managing acute kidney injury and associated hyperkalemia. He brings more than 15 years of clinical expertise to his work.
The team utilizes advanced diagnostic approaches and personalized treatment protocols, including emergency dialysis services and continuous renal replacement therapy for critical cases. Their coordinated care plans focus on both immediate stabilization of dangerous electrolyte imbalances and long-term kidney function recovery.

